The USA Leaders | May 18, 2026
Who declared the Ebola outbreak a global health emergency?
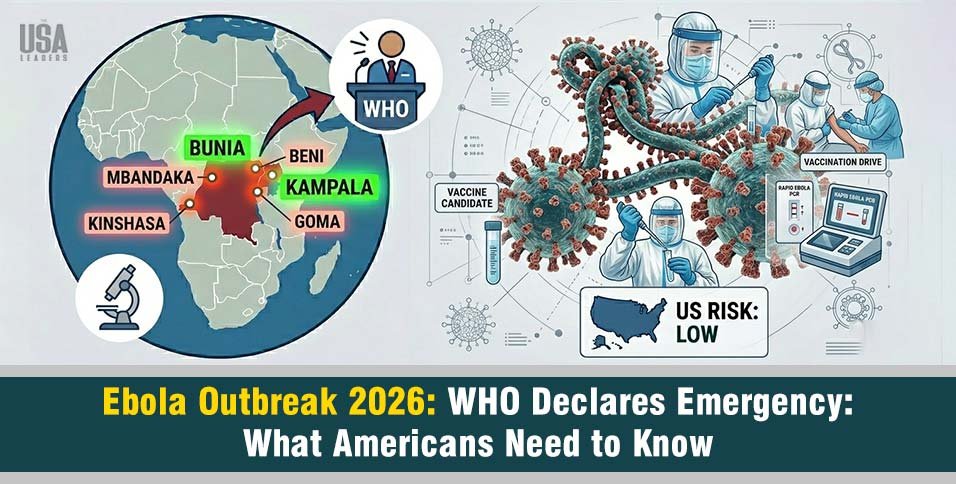
WHO Director-General Tedros Adhanom Ghebreyesus declared the 2026 Ebola outbreak a Public Health Emergency of International Concern (PHEIC) on Sunday, May 17, 2026, after more than 300 suspected cases and 88 deaths across the Democratic Republic of Congo (DRC) and Uganda.
Quick Facts: The 2026 Ebola Emergency at a Glance
| Detail | Official Status & Data Point |
| Who declared the emergency? | WHO Director-General Tedros Adhanom Ghebreyesus |
| Date of declaration | May 17, 2026 |
| Pathogen causing outbreak | Bundibugyo virus (A rare species of Ebola) |
| Primary countries affected | Democratic Republic of the Congo (DRC) and Uganda |
| Cities with confirmed cases | Bunia, Rwampara, Mongbwalu (DRC); Goma, DRC (conflict zone rebel-held); Kampala (Uganda) |
| Current Toll (Africa CDC) | 336 suspected cases; 88 reported deaths |
| Ebola death rate (Strain) | Approximately 25% to 50% |
| Approved vaccine available? | No, existing vaccines do not protect against this strain |
| Risk to the United States | Low, according to the CDC |
| Is this a global pandemic? | No, it does not meet pandemic criteria; borders remain open |
WHO Declares Global Health Emergency — The Alarm Is Real, But Here’s the Context
On May 17, 2026, the World Health Organization issued its highest health alert. The Ebola outbreak in the Democratic Republic of Congo and Uganda was declared a Public Health Emergency of International Concern (PHEIC).
This is the strongest warning the WHO can give short of calling a pandemic the same level used during COVID-19. However, the WHO stressed that this outbreak is not a pandemic yet. Borders should remain open, and daily life should continue.
The alert is meant to push governments and health agencies to act quickly, not to cause public panic.
In Which Cities Have Laboratory-Confirmed Cases Been Reported?
Tracking the Ebola outbreak map for 2026 focuses on major transport routes and busy commercial areas. The virus spread beyond remote villages because it initially affected a highly mobile population in regional gold-mining centers.
Laboratory-confirmed cases of the Bundibugyo virus are currently reported in the following urban locations:
- Mongbwalu (DRC): A high-traffic mining zone in the Ituri Province where the outbreak was first detected after an unusual cluster of healthcare worker deaths.
- Bunia (DRC): The capital city of Ituri Province. Sick individuals migrated here from rural zones seeking advanced medical care, creating an urban transmission risk.
- Rwampara (DRC): A critical health zone right outside Bunia, where health teams confirmed the first wave of positive laboratory samples.
- Kampala (Uganda): The capital city of neighboring Uganda. Two unlinked, imported cases were confirmed in travelers who arrived directly from the DRC, forcing international intensive care units into immediate isolation protocols.
Note on Kinshasa: An initial case was reported in DRC’s western capital, but subsequent confirmatory testing by the INRB returned negative. Kinshasa is not a confirmed transmission site.
Decoding the Pathogen: How Does the Bundibugyo Virus Compare to the 2014 West Africa Strain?
Most people think Ebola is just one disease, but it is actually a group of different virus strains. Knowing which strain is spreading helps doctors choose the right treatments and control methods.
The Ebola Vaccine Dilemma
During recent outbreaks, response teams used the Ervebo vaccine to successfully stop the spread. However, this vaccine only works against the Zaire strain of Ebola and does not protect against the Bundibugyo strain. At present, there is no approved vaccine or specific treatment for Bundibugyo. Doctors can only offer supportive hospital care, so health teams must rely on traditional containment measures to control the outbreak.
Analyzing the Ebola Death Rate
Although there are limited medical treatments, this virus is less aggressive than other Ebola strains. The Bundibugyo Ebola virus has a death rate of about 25% to 50%. While it is still very dangerous, it is far less deadly than the Zaire strain, which reached mortality rates of up to 90% during the 2014 West Africa outbreak.
Here’s how the 2026 outbreak compares to the largest Ebola crisis in history:
| Feature | 2014–2016 West Africa | 2026 DRC/Uganda |
|---|---|---|
| Strain | Zaire ebolavirus | Bundibugyo virus |
| Ebola death rate | Up to 90% | 25–50% |
| Peak confirmed cases | ~28,616 | 336+ suspected (growing) |
| Approved vaccine | Developed during outbreak (Zaire only) | None |
| Approved treatment | Yes (Zaire only) | None |
| Cross-border spread | Yes (US, UK, Spain) | Yes (Uganda confirmed) |
| WHO emergency declared | Yes (2014) | Yes (May 17, 2026) |
| Detection speed | Faster, higher media attention | Delayed ~3 weeks |
Ebola Spread Timeline: How This Outbreak Went Undetected for Weeks
One of the most worrying parts of this outbreak isn’t the virus itself, but how long it spread without being detected.
The first suspected case was a 59-year-old man who showed symptoms on April 24, 2026, and died three days later. However, health authorities were not alerted until May 5, and the alert came from social media, not hospitals. By then, 50 people had already died.
Early lab tests failed to detect the virus because they only checked for the Zaire Ebola strain, not the Bundibugyo strain. The correct tests were used later, and the first Bundibugyo case was confirmed on May 14, nearly three weeks after the first death.
Health experts say cuts to global disease surveillance may have delayed detection, allowing the outbreak to spread faster.
When the outbreak was officially declared on May 17, it had already reached at least nine health zones in the DRC and spread into Uganda.
Ebola Outbreak 2026 Map: Where Is the Virus Right Now?
The outbreak is mainly concentrated in Ituri Province in northeastern DRC, near the borders of Uganda, South Sudan, and Rwanda. This area has a history of Ebola outbreaks, including the world’s second-largest outbreak from 2018 to 2020. Early cases were wrongly identified by standard Zaire test kits, allowing the virus to spread for nearly three weeks. On May 14, advanced testing confirmed the Bundibugyo strain. In Ituri, health officials are closely monitoring major travel routes to prevent further spread.
- Neighboring health zones directly bordering South Sudan.
- Heavy transit pathways leading toward North Kivu Province (Goma).
- Commercial flight corridors connected to Kampala (Uganda’s capital).
The 2018–2020 outbreak was worsened by the ongoing armed conflict, which is still unresolved. These same security issues are likely to make the current response difficult as well.
From Ituri, the virus has traveled along human movement routes to:
- Other health zones within Ituri Province
- North Kivu Province (Goma)
- Kinshasa (DRC capital, far west of the country)
- Kampala (Uganda’s capital)
The WHO has clearly stated that because many test samples are positive and cases are spread across multiple regions, the actual size of the outbreak is likely bigger than what current data shows.
How Does the Bundibugyo Virus Compare to the 2014 West Africa Ebola Strain?
The 2014–2016 Ebola outbreak in West Africa was the largest ever recorded, causing nearly 29,000 cases and over 11,000 deaths in Guinea, Liberia, and Sierra Leone. The virus also spread briefly to the United States, Spain, and the United Kingdom.
The outbreak was caused by the Zaire ebolavirus, the most deadly strain. Below is a comparison with the current Bundibugyo outbreak.
| Feature | 2014–2016 West Africa | 2026 DRC/Uganda |
| Strain | Zaire ebolavirus | Bundibugyo virus |
| Ebola death rate | Up to 90% | 25–50% |
| Total confirmed cases (peak) | ~28,616 | 336+ suspected (growing) |
| Approved vaccine | Developed during/after (for Zaire only) | None |
| Approved treatment | Yes (for Zaire only) | None |
| Cross-border spread | Yes (US, UK, Spain) | Yes (Uganda confirmed) |
| WHO emergency declared | Yes (2014) | Yes (May 17, 2026) |
| Detection speed | Faster, more media attention | Delayed by ~3 weeks |
The main difference is that this strain is less deadly, but there are no medical treatments or vaccines for it. It also spread for three weeks before anyone knew, and both points are important.
Past Bundibugyo Outbreaks: This Has Happened Before Twice
This is the third time the Bundibugyo virus has appeared in this region, and the pattern is clear:
- First outbreak (2007–2008, Uganda – Bundibugyo district): The virus was first discovered in western Uganda. It infected 149 people and caused 37 deaths. The virus was named after this district.
- Second outbreak (2012, DRC – Isiro): The next outbreak happened in northeastern DRC. There were 57 cases and 29 deaths, and it was brought under control fairly quickly.
- Third outbreak (2026, DRC and Uganda): This is the largest Bundibugyo outbreak so far, with hundreds of suspected cases and spread into two capital cities. The increase in scale compared to 2012 is significant.
This outbreak is also the 17th Ebola outbreak in the DRC since the virus was first identified there in 1976. While this history is concerning, it also means the country has strong experience in responding to Ebola, offering some cautious hope.
Ebola symptoms: what to watch for
Key symptoms — Bundibugyo virus disease
| Symptom | Typical onset |
| Sudden fever | 2–21 days after exposure |
| Severe headache | Early (day 1–3) |
| Muscle pain and weakness | Early (day 1–3) |
| Vomiting and diarrhea | Day 3–5 |
| Abdominal (stomach) pain | Day 3–5 |
| Unexplained bleeding or nosebleeds | Later stage (day 5+) |
| Vomiting blood | Later stage (day 5+) |
What’s the Risk to Americans — and Are Any US Citizens Exposed?
The CDC’s official position, as of May 17, 2026: the risk to the American public remains low.
This isn’t spin. Here’s the science behind it:
Ebola does not spread through the air. You cannot get it from sitting near someone on a plane, being in the same building, or through casual contact. The virus spreads only through direct contact with bodily fluids such as blood, vomit, urine, or sweat of a person who is sick or has died from Ebola.
Importantly, a person with Ebola is not contagious until symptoms appear. This means a traveler who flies before showing symptoms does not pose a risk to others on the plane.
However, Americans should stay informed. According to STAT News, several U.S. citizens in the Democratic Republic of the Congo may have been exposed to Ebola, and at least one is suspected to have symptoms. The U.S. government is reportedly arranging medical transport so exposed individuals can receive care under strict quarantine.
The CDC has also posted:
- A Level 2 travel notice for DRC (Enhanced Precautions)
- A Level 1 travel notice for Uganda (Usual Precautions)
How the CDC and Global Health Community Are Responding
The global response began quickly once the outbreak became clear, although health experts say it started later than it should have.
What the CDC is doing right now:
- Activated its Emergency Response Center
- Deployed staff through its in-country offices in DRC and Uganda
- Supporting surveillance, contact tracing, lab testing, and infection prevention
- Mobilizing additional teams from the CDC headquarters in Atlanta
- Conducting exit screening at airports in DRC and Uganda because people with Bundibugyo are only contagious when symptomatic, exit screening is a meaningful line of defense
What the WHO is doing:
- Convening an emergency committee to advise on international response
- Coordinating with DRC and Uganda health ministries
- Providing field support to affected communities
What NGOs are doing: Organizations like Médecins Sans Frontières (MSF/Doctors Without Borders) are preparing large-scale field responses as quickly as possible.
The ways to stop Ebola without a vaccine are well known: quickly track contacts, isolate infected people, protect healthcare workers, and involve local communities. These methods have worked before. In 2019, the WHO controlled a larger outbreak in the DRC using the same approach.
What Should Americans Do Right Now? A Practical Guide
No travel plans to DRC or Uganda
Stay informed by monitoring CDC and WHO updates. No changes to daily life are needed. The risk of Ebola reaching US soil remains very low at this time.
Planning travel to DRC
Check the CDC Level 2 travel notice before departure. Avoid all contact with sick people, deceased individuals, and wild animals in the region. Know the symptoms listed above and carry the CDC hotline number.
Recently returned from DRC or Uganda
Monitor your health for 21 days after your return. If any symptoms appear, call a healthcare provider immediately and tell them your travel history before you walk in, so they can prepare proper isolation.
Healthcare workers treating a possible case
Apply full isolation protocols immediately. Notify your local public health authority before the patient is moved. Follow CDC’s infection prevention and control recommendations for viral hemorrhagic fevers.
The Bottom Line
The WHO’s declaration is a serious warning based on facts. It is not a reason to panic, but it is a clear reason to stay alert.
The outbreak spread for three weeks because proper tests were not used, and monitoring systems failed. It has now reached two capital cities, and there is currently no vaccine or approved treatment.
The world knows how to stop Ebola. The real question is whether action can be taken quickly enough in a conflict-affected region with enough resources. History shows it is possible, but only with urgent action, strong coordination, and sufficient funding.
For most Americans, the immediate risk remains low. However, the coming weeks will be critical in determining whether the outbreak slows down or spreads further. You can follow confirmed, daily-updated case numbers on the CDC’s Ebola Situation Summary page.
Also Read – MV Hondius Hantavirus Outbreak: 17 Americans Evacuated to Nebraska